By Dr. Chow Sze Loon
Battling the new lineup of COVID-19
As the nation grapples with the resurgence in COVID-19 infections, the much-anticipated national COVID immunization program (PICK) has slowly picked up its pace since Feb 2021.
Many did expect the long-awaited vaccine as the silver bullet to end the ongoing pandemic, but the reality presents a new, unexpected formidable lineup of Variants of Concern (VOCs) with the Delta variant being the most transmissible.
Besides that, the number of COVID-19 related deaths associated with silent hypoxia which often leads to Brought in Dead (BID) cases are alarming.
Silent hypoxia, a condition where the patient has alarmingly low oxygen saturation levels without exhibiting any typical breathing difficulty.
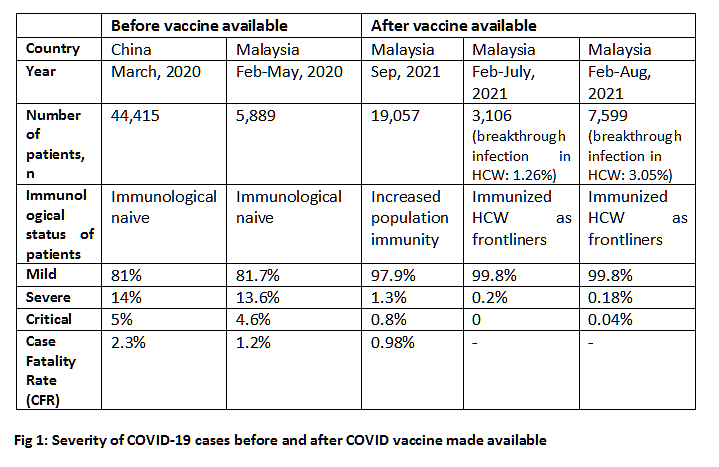
Growing evidence suggesting improvement in clinical outcomes post COVID vaccine
In early 2020, the clinical presentation of COVID-19 reported in China and Malaysia were similar as majority of the immunological naive patients presented with mild symptoms.
Half a year into PICK, low-risk patients contribute up to 98% of the total positive cases and are usually allowed for home isolation.
Vaccination aims at reducing the risk of long COVID complications and deaths.
 Is integrated CAC on the cards or just a wish list?
Is integrated CAC on the cards or just a wish list?
Targeted mass testing by state government (Penang Saring COVID-19) and compulsory biweekly RTK-Ag testing by MITI have contributed to the surge of positive cases in a short period of time.
Recognizing RTK-Antigen as confirmatory test has made immediate case detection and isolation possible.
CACs, headed by Family Medicine Specialists (FMS) are confronted with two main limitations in expanding its current capacity: manpower and space.
Delay in isolating patients would suggest the main purpose of RTK-Ag as confirmatory is not achieved.
While PICK is having good collaboration with private sectors at all levels, CACs are manned by MoH singlehandedly since early 2021.
Penang has been reporting around 1,700 positive cases per day, 98% of it (1,666) are low risk category for home isolation. It means additional 333 patients daily to be monitored by CAC in each district! Hence, the bottleneck in public health response is not unexpected.
Rapid identification (RTK-Ag) and referral to CAC for assessment on the same day for immediate isolation, bypassing the usual investigation and tracing is crucial for high-risk individuals.
In short, the F-T-(I-T)-S would be more practical, relevant for current scenario, pushing for rapid detection of cases and isolation before tracing the close contact.
Comments on PKRC shared in social media do not usually help in advocating for isolation. Regardless, isolation is to break the chain of transmission.
Close health monitoring would help in delivering prompt medical attention for high-risk patients. Alternative integrated CACs managed by non MOH would give these patients a choice, preventing further congestion in current CACs.
Such integrated CACs may model upon the modus operandi in recruiting private practitioners in operating PPV Integrasi, carrying out the physical/virtual assessment for these patients.
Those paying out of pockets and B40 community with some subsidy in place are the potential clients for such integrated CACs.
To date, up to 70 hotels nationwide have been given the green light and are ready to house low-risk COVID patients.
Inappropriate isolation defeats the purpose of periodic testing
MITI has recently mandated employers to do biweekly RTK-Ag as a proactive measure to curb workplace transmission.
While such initiative is commendable, it may not be effective should the hostels and living condition for foreign workers are not improved.
As of April 2021, up to 74% of employers were found not providing proper housing for the workers. Besides that, periodic screening without prior identification of site for isolation (of positive cases) and quarantine (of close contact) for the workers may just hamper the ultimate goal.
Additional PPE such as face shields should be considered in workplace setting that require prolonged face to face interaction especially when most of the employees are not fully vaccinated.
For optimal protection against respiratory virus, face shield should extend below the chin, to the ears at both sides, and there should be no exposed space between forehead and the shield’s headpiece.
Double-masking with the combination of a fabric mask over an interior surgical mask, along with a face shield offers greater protection compared to wearing either one of those.
Protection against exposure to highly contagious Delta variant is as high as 96% with additional barrier for the eyes.
Enhancing ventilation in enclosed work spaces must be a priority and a routine practice.
Empowering patient for self-care and monitoring
About 3.5% of low-risk patients may deteriorate into category 4-5 with warning signs.
Thus, patients need to be empowered to self monitor and report those warning signs (e.g.: persistent or new onset fever, extreme fatigue, respiratory compromise, profuse sweating, blue lips or change of color in the skin) in MySejahtera app besides being followed up by CAC.
Home pulse oximeter is safe, non-invasive way to assess oxygen saturation in the blood.
MDA has approved pulse oximeter as an essential tool for patients undergoing home isolation to identify the need for medical evaluation, oxygen therapy or hospitalization even before the onset of warning signs to prevent silent hypoxia (as per WHO interim guidance, 12 Aug 2020).
Therefore, calling for a ceiling price for such essential device is appropriate.
High-quality equipment consistently provides results within minimal margin (+/-2%). However, factors such as movement, temperature, or nail polish are known to impact its accuracy.
Baseline oxygen saturation should be known (SpO2 ≥ 95% is normal). Some practical breathing exercises, rehabilitation tips and self-management after COVID related illness can be obtained from WHO self-management leaflet.
The Occupational Therapy Unit under Penang General Hospital also produces video to demonstrate effective breathing techniques as well as guide on self proning which would help patient to improve the breathing comfort and oxygen level.
Self isolation is a social responsibility for the purpose of public health. That requires awareness and discipline, though continuous enforcement does play a role.
Non-pharmacological interventions applied globally are rather similar, notwithstanding the timing of implementation. The main difference is perhaps the compliance of these measures which ultimately fall back to the discipline and awareness of its society.
Finally, it is high time for all stakeholders to recognize and accept digital Home Surveillance Order (HSO) as part of digitalization initiative.
Such effort is not just environmental friendly but time saving for patients and healthcare provider.
Reference:
1. The severity of diagnosed COVID-19 cases in China (*Death Rate is based on CONFIRMED CASES. This value can not possibly represent an accurate percentage since only the sickest people are tested for COVID-19)
2. Sim BLH, Chidambaram SK, Wong XC, Pathmanathan MD, Peariasamy KM, Hor CP, Chua HJ, Goh PP. Clinical characteristics and risk factors for severe COVID-19 infections in Malaysia: A nationwide observational study. Lancet Reg Health West Pac. 2020 Nov;4:100055. doi: 10.1016/j.lanwpc.2020.100055. Epub 2020 Nov 17. PMID: 33521741; PMCID: PMC7837062.
3. KP Kesihatan: Kenyataan Akhbar KPK 23 Ogos 2021 – Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia
4. Facebook: Noor Hisham Abdullah
(Dr, Chow Sze Loon is a medical specialist trained in public health, former state public health surveillance officer involved in surveillance, preparedness and response activities on infectious diseases outbreak, crisis, disaster and emergency in Penang.)
ADVERTISEMENT
ADVERTISEMENT